Tell us about your book When Antidpressants Aren’t Enough and what inspired you to write it.
This book is derived from over 10 years of research on how to treat people who have been treated with antidepressants, the most common form of depression treatment, yet failed to fully recover. This is an unfortunately common occurrence. In the largest study of people treated with antidepressants, the STAR*D study, only one-third of people treated for 12 weeks recovered and after a second course of treatment one-half had recovered. This means that 50% of people still suffered significant depression despite two full treatments which is often more than most people receive. I developed the Practicing Alternative to Heal Depression study (PATH-D) to see if we could teach people mindfulness-based cognitive therapy (MBCT) to offer them an empowering technique that they could use to heal themselves. The results showed significant benefits in reducing depression levels in this randomized controlled trial sponsored by the National Institutes of Health.
What can people who fail to fully recover from depression with antidepressants do?
This is a common occurrence. In our study participants averaged 7 years of suffering after two or more antidepressant trials. There are a range of things such people can try. These include additional medication trials or trying various forms of psychotherapy or even electroconvulsive treatment or transcranial magnetic stimulation. Our research indicates that MBCT is a particularly effective technique that people can learn over 8 weeks. It provides a method for people to have a skillset that they can utilize on their own to deal effectively with depression.
What is Mindfulness Based Cognitive Therapy (MBCT)?
MBCT is a blend of some aspects of cognitive behavior therapy with mindfulness meditation. Mindfulness meditation is an ancient Buddhist technique that has been secularized so it can be used by all people regardless of their background. It teaches that in depression thoughts are often negative ones like “I’ll fail at whatever I try”. I’m not good enough” or “I’ll never get better”. In MBCT, you learn that such ideas are just thoughts, not facts.
You say in the book’s introduction that you aim to help readers change their relationship to depression. How so?
In traditional cognitive behavior therapy, you are taught to try and answer back to negative thoughts. This can be challenging because if you have been depressed for a long time you tend to believe the negative thoughts. In MBCT you learn a different approach. One by learning how to focus your attention you can let go of negative thought. For example if you can learn to focus on your breath, there is no bandwidth available to focus on negative thoughts. Secondly, MBCT is focused on the present moment. If you are focused on the present moment you let go of ruminations about the past or anticipation about the future. This is important because in depression you are often focused on past regrets and losses while with anxiety you are focused on upcoming catastrophes. Focusing on the present moment has a natural antidepressant and antianxiety effect.
How has your own relationship with depression informed your work?
With my first experience with depression I tended to believe the negative thoughts when they occurred. For example, when I felt guilty I tried to figure out why I was feeling that way. Had I down something in the past that warranted guilt? As I became more mindful, I realized such negative thoughts were symptoms of depression not facts that had to be investigated as actual realities. Moreover I began to see depressive moods as being similar to the weather. For example, if it is raining out today, it may mean I can’t go on a picnic but I realize it is a transient event and I can pursue alternatives for the day. So when I experience depression I can realize it is transient and not be completely flattened by it.
You say in the book that when a depressive episode hits that it is important to see them for what they are: recurrences of an illness and not a personal weakness or moral failure. Tell us more about that please.
When depression hits, as part of the syndrome, you are often filled with self-recriminations. There is a tendency to blame yourself and see yourself as having a personal weakness or failure. This is a rather specific aspect of reaction to an illness. You don’t see people with asthma or diabetes blaming themselves when they have an exacerbation. With a mindfulness approach you learn to accept things as they are. Winston Churchill embodied this approach when speaking of his depression; he said “the black dog is back today”
Are there ways to prevent relapse once you have recovered from depression?
MBCT was originally developed as a relapse prevention technique. In studies comparing it to treatment as usual (no specific treatment), it was twice as effective in preventing relapse over a one year period. More importantly in a larger study, MBCT was compared to maintenance antidepressant treatment, the most common approach to relapse prevention. In one study it was just as effective. In fact, there was some evidence to suggest that a greater severity of depressive symptoms prior to treatment was associated with even less relapse with MBCT compared with antidepressants
These studies indicate that the techniques of MBCT such as focusing attention, decentering (distancing yourself) from negative thoughts and feelings, and being compassionate towards yourself can have powerful effects in preventing depression and limiting its impact when it does recur.
You say that negative thoughts are not facts but rather symptoms of depression itself. Please elaborate.
Depressive moods generate negative thoughts and vice versa. When you have a negative thought like “I’m no good” if you can realize it’s a symptom of depression and not a fact, there is an antidepressant effect to that understanding. It’s like realizing that an elevated fever is part of having pneumonia and not a fundamental metabolic disturbance. One way of looking at depressive thoughts is by imagining them being like items in store windows as you walk down the street. You can observe them but you don’t have to go in the store and buy them. You can view the negative thoughts as just thoughts but not something you have accepted as facts.
You also say that in mindful approaches to depression, the key is not to find the origins of negative feelings, but to change our relationship to them, so they no longer have significant power in our lives. Can you give us an example of what this looks like in real life?
There is an ancient Buddhist story about a warrior shot in the chest with an arrow. He asks his colleagues “who shot the arrow?” , “why did they aim it at me?”, and “where was the arrow made?”. In this situation it is more important to get the arrow out rather than focus on answering such questions. With mindfulness, you learn to shift your attention from answering questions about the origins of your depressive experience to focusing on the present moment. As you do this, negative thoughts and feelings can shift into the background. This is similar to a radio playing with the volume turned down. The depressive mood and thoughts may still be present but they don’t occupy center stage.
How would you definite mindfulness?
Mindfulness at its core is being aware of your experiences as you are experiencing them and suspending judgment about them. These include sensations, thoughts, and feelings. Mindfulness meditation can be thought of as shining the spotlight of attention on a specific focus that you select in the present moment. This spotlight can be as broad or narrow as you like. Typically mindfulness can be thought of in two ways. In one, the discrete form, you practice focusing your attention for a specific amount of time, say a meditation where you focus on your breath for 10 minutes. When your mind wanders you notice the wandering and bring the attention back to the breath. In the other form of mindfulness, it can be called dispositional mindfulness where you bring a mindful awareness to your everyday life. For example you notice the sensations in your feet as you walk down the street. In both forms of mindfulness you are focusing your awareness but the settings differ.
How does mindfulness help counter depression?
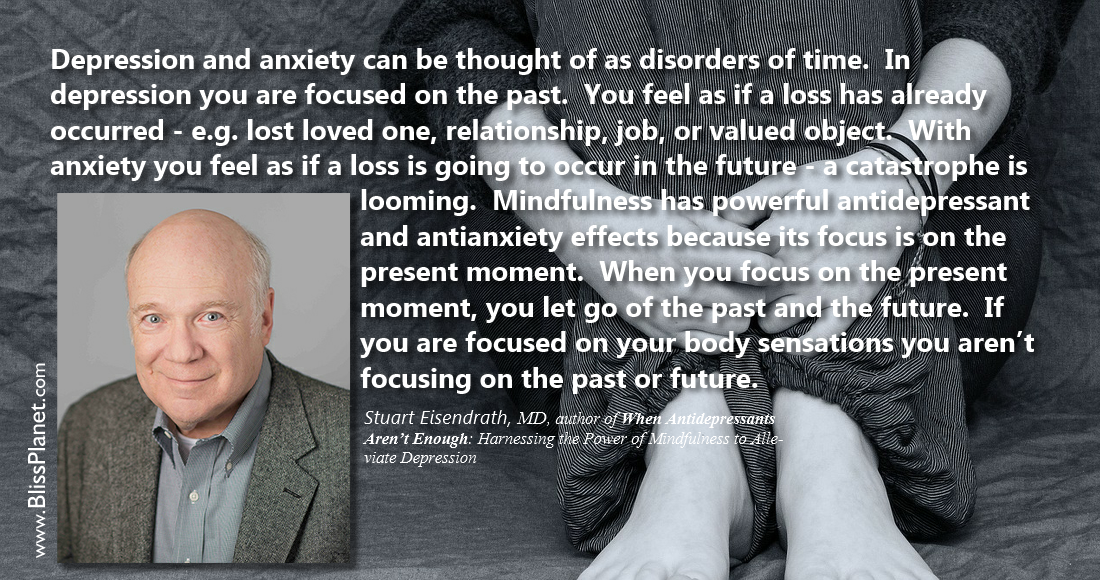
Depression and anxiety can be thought of as disorders of time. In depression you are focused on the past. You feel as if a loss has already occurred—e.g. lost loved one, relationship, job, or valued object. With anxiety you feel as if a loss is going to occur in the future—a catastrophe is looming. Mindfulness has powerful antidepressant and antianxiety effects because its focus is on the present moment. When you focus on the present moment, you let go of the past and the future. If you are focused on your body sensations you aren’t focusing on the past or future.
Can anyone do mindfulness meditation and does it require a big time commitment?
If you can breathe, you can do mindfulness. Mindfulness is a skill like others. When you start learning to build your muscles, you start with small weights and gradually increase them. The same approach applies to mindfulness. You start with short meditations and then learn to vary the types of meditations you do. Many people find that short meditation; say 5-10 minutes a day are easiest to do while other people prefer a 30 minute meditation. There is no evidence that a specific amount of time is necessary to learn mindfulness skills. Rather, it is important for you to develop your own practice of what works for you.
What advice do you have to offer someone who is interested in starting a mindfulness practice with the intention of healing from depression?
If you want to learn mindfulness techniques to heal from depression, MBCT is a proven technique. I’d recommend taking an organized approach. This might be by taking a class or by following the program outlined in the book, When Antidepressants Aren’t Enough. Either way will serve as a guide that can offer a path to healing while helping avoid pitfalls.
Tell us about the science behind Mindfuless- Based Cognitive Therapy (MBCT)?
MBCT not only has powerful psychological effects, it also has effects on the brain itself.
In the PATH-D study we investigate participants by looking at how their brains functioned before and after treatment. We did this by using functional magnetic resonance imaging of the brain. This technique shows second by second changes in the brain. In our studies, we found that areas of the brain associated with emotion regulation were enhanced while areas of the brain associated with emotion production—such as anxiety and depression—were reduced. Although research on the effects is still being investigated, it is clear that MBCT has definite brain effects. These effects appear to reverse the changes typically found in depression.
What do you hope readers will take away from your book?
I hope readers will gain a better understanding of depression including both its effects and ways of dealing with them. I hope that readers will learn to treat themselves with more self-compassion in realizing depression is a widespread illness. It is not a moral weakness or personal failure. There are new and powerful techniques like MBCT that offer hope in healing depression and empowering the individual with skills that they can utilize rapidly and effectively.
Stuart Eisendrath, MD, is the author of When Antidepressants Aren’t Enough and the founding director of the University of California San Francisco Depression Center. A senior clinician and research psychiatrist at UCSF, his lectures on mindfulness-based cognitive therapy for University of California TV have been viewed more than 1.5 million times. Visit him online at www.stuarteisendrath.com
WHEN ANTIDEPRESSANTS AREN’T ENOUGH
October 1, 2019 • Psychology/Self-Help • Paperback & eBook • 224 pages
Price: $18.95 • ISBN 978-1-60868-597-4
Special thanks to New World Library
Author: Bliss
Dedicated to making a positive difference for people, animals, and this beautiful planet!